Manage Profitably (With Less Headaches, Less Stress and More Time for Patient Care)
(Reprinted from Podiatry Management Magazine - January 2018 Issue, pg. 81-88)
Lynn Homisak, PRT, CHC
“Managing my practice is exhausting! I just want to practice podiatry and take care of my patients!”
Can you relate? If yes, you are not alone. Practice owners all across the country would agree that the burden of every day management weighs heavily and requires more attention than perhaps they might have imagined. In fact, if you are one of them, it’s very possible the minute you stepped into those “ownership” shoes and hired your first employee, you probably concluded that critical lessons were missing from the curriculum in podiatry school. Or, you missed that class. You know, the one where the instructor revealed all the skills you need to properly handle people, money and processes. If you didn’t realize it then, you learned quickly just how crucial this knowledge is in operating a successful business.
It is no secret that poorly run offices are often the result of poor or absent management. They never seem to reach acceptable levels of functionality, efficiency, productivity and that word we all love – profitability! I’d like to share with you some specific, yet ridiculously SIMPLE strategies and present a scientific theory that could play a major role in practice life as you know it. It will not only give you better control of your practice through more awareness; it will also encourage healthier overall performance with fewer headaches. We’ll get to the “how-tos” of improving key areas that lead to practice excellence. First, let’s tackle that “exhaustion” problem.
WHY are you are exhausted?
We know that quality of sleep, types of food we eat, and physical activity play a significant role in regulating energy levels. However, we must also factor in cognitive load – the total amount of mental effort being used in your working memory. Our brains store a limited capacity of cognitive load and every time we make a decision – large or small – (in this case, sorry, size does not matter), we reduce this stored amount. Think of a fully charged cell phone. Each time we call, text or surf, the percentage of battery power decreases. Same holds true with cognitive load.
Here’s what is important. Our working memory is vulnerable to overload, and the onslaught of (unnecessary) decisions places excessive demand on it, draining that daily memory ‘bank’. Decision overdose on a daily basis can lead to mental exhaustion leaving you with executive function fatigue, impaired judgements and lower performance. You are a race car running on fumes. This overload can result in: 1) making irrational, impulsive decisions, 2) postponing critical decisions; or 3) avoiding decisions altogether. None of which are useful in management.
Imagine each morning you are given a bucket filled with marbles representing your daily quota of cognitive load. It is all you’re going to get for the day. Every time you make a decision, whether at home or work, one of those marbles disappears from your bucket. Now, if you are the type that insists only YOU are “The Decider” for every little thing in the office, you will “lose your marbles” faster than you can say “meltdown”, leaving you with minimal to zero mental effort by day’s end.
Wait. Don’t think you make a lot of decisions? Surprise! Between getting up in the morning and going to bed in the evening, the average person makes approximately 35,000 decisions. Over 200 of those are just food choices! Should I eat now or later? Red clam chowder or white? Does it need salt? Pepper? Crackers? Sandwich with that? Half or whole? What Kind? Mayo or Mustard? Condiments? On wheat? Rye? Sourdough? White? Semolina? Toasted? Is it gluten free? How about dessert? Cake? Pie? Coffee? Tea – hot or iced? Sugar or Sweet-n-Low? Milk or cream? Well, you get the picture. That’s a lot of marbles!
Decision Fatigue
Let’s look at how a typical day might play out.
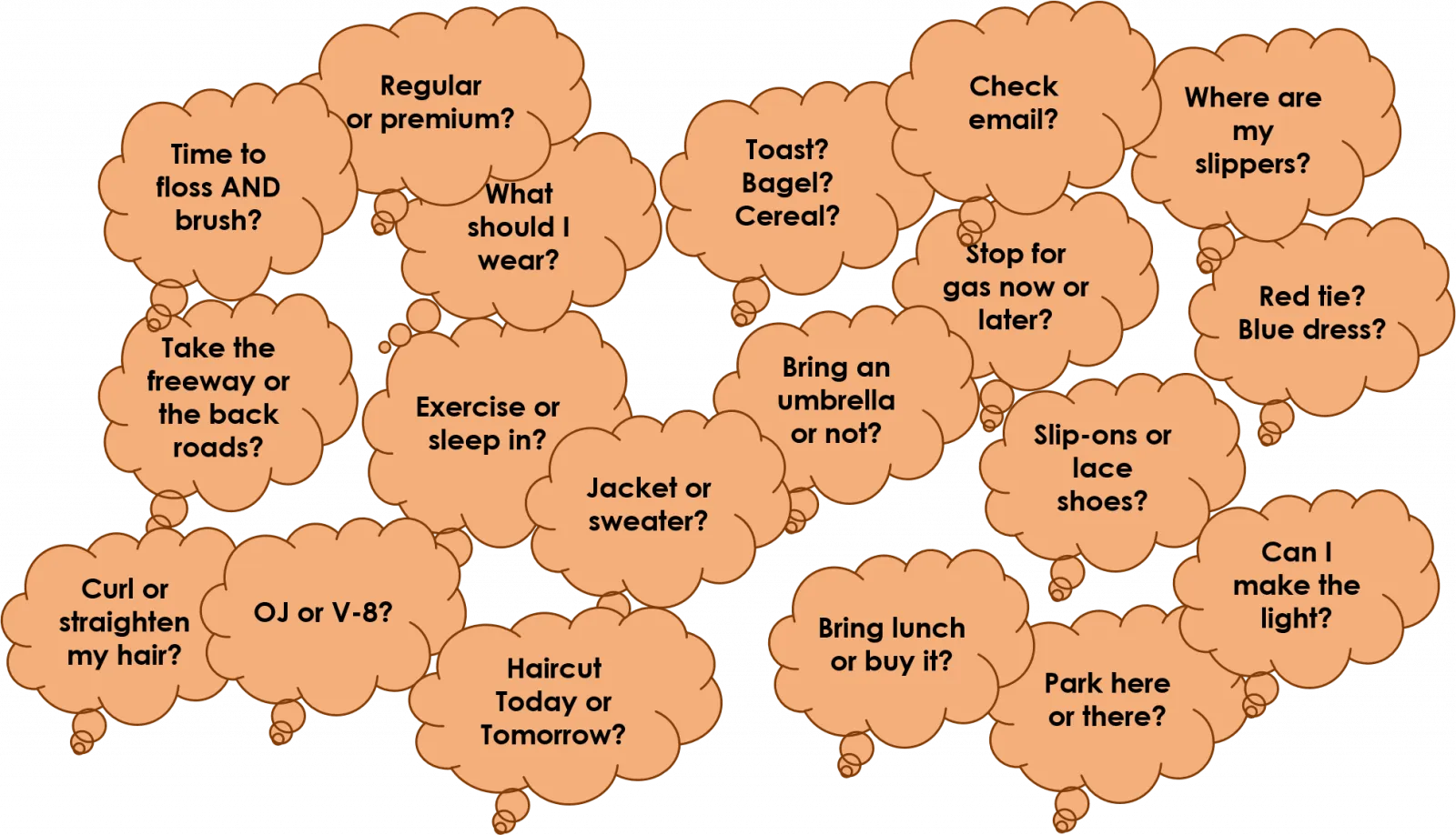
(Figure 1) You wake up and before even positioning your two feet on the floor, decision wheels are already in motion. In fact, you’ve put a pretty healthy dent in your daily bucket of marbles before you even get to work, many times without even realizing it. For example, should I floss, what to wear, juice or coffee? Even the duration at a stop sign is, that’s right, another decision.
(Figure 2) At work, more decisions await you – some minor, others critical/clinical ones. Remember, the magnitude of each decision doesn’t matter in the draining process and the assault on your marbles continues.

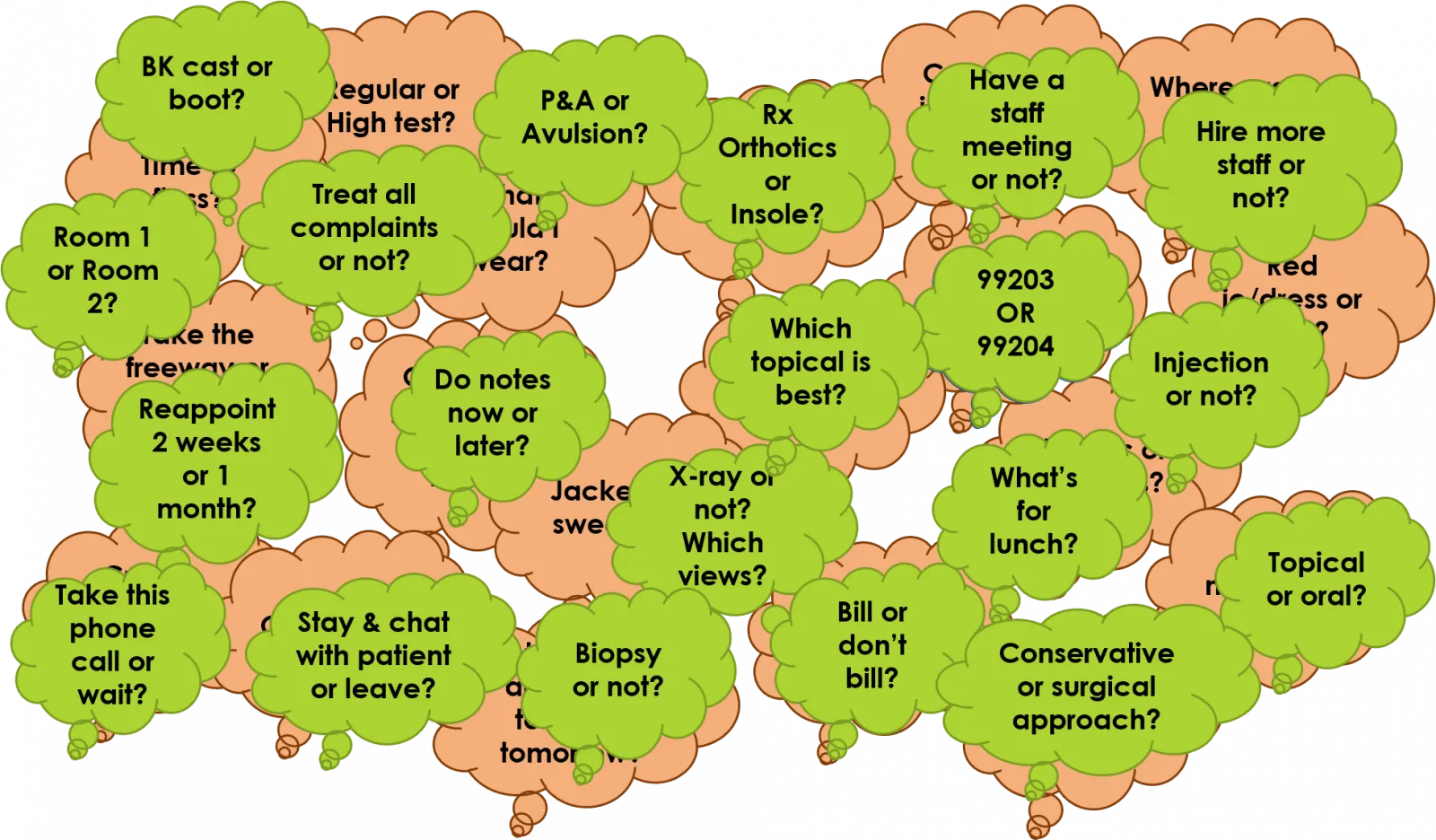
(Figure 3) As your day progresses, your staff comes to you with questions that steal even more of your attention (as do patients, drug reps, visitors, phone calls, etc.). Dealing with decision after decision takes its toll. There is a run on the ‘bank’; your bucket is empty; you have lost all your marbles; exhaustion triumphs; and the day isn’t even half over. Two aspirins, please.
“So, okay, decision making is part of owning a business. That’s a given. What does all this have to do with my profitability & efficiency?”
What if I told you that reducing the number of decisions made on a daily basis could likely increase profitability and productivity; reduce everyday practice management stress; and give you more time to do what you enjoy? Would you be willing to change the way you do things to realize these prized benefits?
It’s About Time
A physician’s time can be categorized in one of three ways - productive, delegated or voluntary. When I go into a client’s office, one of the first things that jumps out at me is how many doctors insist on doing all patient care tasks themselves. I might see a physician leave a treatment room to fetch a DME product out of the lab or use their productive ‘doctor’ time to fit a patient with a night splint, or explain stretching exercises. And almost without fail, I witness docs seeking to locate the crafty, ever-elusive ‘ staffamongus ’ by shouting down the hall or repeatedly pressing the room status button for assistance/assistants. Where are they? Why aren’t they here?
The tasks mentioned above realistically don’t require a medical license and can easily be performed by trained staff or physician extenders. That some doctors want to pitch in during crunch times is understandable, even considerate. When these actions become the norm, however, “productive” time is threatened. Remember, the objective is to ease cognitive fatigue by reducing overload. Eliminate unnecessary tasks to eliminate unnecessary decisions. Bottom line, it makes sense for doctors to concentrate on “doctor-only” duties. The chef seldom washes dishes. The pilot rarely serves coffee.
Quality vs. quantity
A two-year national study by Thompson & Associates [1] shows that every single minute the DPM burns has a value attached ranging from approximately three to eight dollars. So, while leaving your patient to fill an injection or grab a boot may only take a minute, do the math! Minutes over the course of a day, week, month, and year amount to a significant loss of revenue.
Of course, if you choose to “volunteer” for peripheral tasks because you enjoy doing them; by all means, continue. It’s your practice! Just realize that it is an “either-or” situation. Either use productive time throughout the day doing staff work and feeding decision fatigue, or use that time saved to see a few more patients, end the day sooner, spend time with family, enjoy activities, or just relax. It’s not the amount of time you spend with your patients as much as it is the quality of the care they receive.
The “How-tos”
First, routinize!
In order to routinize, you must identify responsibilities that are not routine; yet, still require your input. For example, hiring, training, employee rules, codes of behavior, meetings, billing & collections, scheduling, and preferred treatment prep. Develop Standard Operating Procedures (SOPs) for each of them. SOPs put everyone in the office on the same page and lead to consistent, expected outcomes without micromanaging . This, in turn, saves you time and energy to do what you are most qualified to do – doctoring! Yes, SOPs take time up front to develop; then become the gifts that keep on giving.
Strategic tools like note taking, checklists, “to do” lists, policy and procedural manuals, huddles, and job descriptions are also must-haves that help your team adapt (and stick) to new routine. Management gold!
Second, develop a first-class training program for staff
There are many reasons why some staff do not reach full potential; one of the most common is little opportunity from a lack of training.
If doctors want the kind of staff that are the envy of every office, there is no getting around proper training. Although heaven knows many doctors have tried (and failed) using excuses like:
· “I like doing (this task) and don’t want to give it up”;
· “I’m better at it; I’m faster; I know it will get done right”;
· “It’s not legal”;
· “Staff do not want to do it”;
· “My patients don’t want staff to do it”;
· “If staff are better trained, they’ll expect more money.”
Success comes to those who commit to crafting and participating in their own in-house, top notch training program for ALL staff, including those who claim to be experienced. In fact, it is the experienced ones who usually need to first learn to let go of “the way my other doctor did it” before they can understand your preferred methods.
Effective training programs promote staff retention, self-reliance and uniformity in task implementation. If properly trained, the doctor should be able to step back and let routine do its thing.
Interested in supplemental educational offerings within our profession that can help educate staff? Research the American Society of Podiatric Medical Assisting ( www.aspma.org/certification ) and the American College of Foot and Ankle Orthopedic Medicine ( www.acfaom.org/education-credentialing/certified-clinical-podiatric-medical-assistant-program-ccpma ) for assistant certification programs. Another option, ( www.nailcare-academy.com ), offers courses that train nail technicians in “Cosmetic Podiatry” via online modules, a cash-only ancillary service.
Whether you seek training in management, efficiency and productivity expertise, coding, billing, or product/equipment instruction, various podiatry-staff focused programs are available at select conferences, via webinars or private in-services.
Worried that more knowledge = more pay? Don’t. This is one investment that yields a high ROI. Your employees represent you and your practice. Relying on competent, well-trained personnel to assist in patient care is WORTH it!
The rewards of trained personnel are many. They increase and improve:
• Office efficiency, time management & overall flow;
• Office professionalism;
• Patient perception of their medical TEAM;
• Patient confidence, compliance and customer service; and
• Practice revenue and profitability.
Third, “Delegate and Elevate”
In order to ease the physician’s workload, the general trend is to re-assign duties that can be performed by less costly, properly trained staff. In podiatry, the question that remains blurred is “Which duties can be appropriately and legally delegated?” Without a formal scope of practice for the podiatric medical assistant, some doctors interpret the unwritten “rule” to mean that if they accept responsibility for their staff’s actions, they can delegate anything to them. Many draw the line at invasive procedures, but because this “line” remains ambiguous, other physicians push the envelope and assign duties that actually require a medical license.
Medicare makes clear “extender” qualifications [2] :
· The Physician must personally perform the patient’s initial service and must remain actively involved in patient’s normal course of treatment.
· An extender’s services must be part of the patient’s normal course of treatment.
· The Physician does not have to be physically present in the patient’s treatment room while the services are provided, but must provide “direct supervision,” which means the Physician must be present in the office suite to render assistance, if necessary.
· The medical record should document the essential requirements for Incident-to service.
In a physician office, “Incident-to” services must be provided by someone the enrolled physician or enrolled extender directly supervises, and who represents a direct financial expense to the practice. The supervising provider does not have to be physically present in the room where the patient is receiving services, but must be present in the immediate office suite to render assistance if needed. In a group practice, any enrolled provider that is a member of the group may be present in the office to supervise. The supervising provider is also the billing provider.
Step by step delegation begins by listing tasks you feel comfortable giving up and determining the skill set required to accomplish each one. Then (as noted previously) assign each job on that list to the least paid trained team member who can do it well; feels comfortable and confident performing it; and enjoys doing it. Clarify the job and the expectations in detail and provide necessary tools to successfully complete the task. Finally, offer incentive, praise and reward for quality outcomes and behaviors. Behavior that gets rewarded gets repeated.
Once the physician feels secure in their staff’s knowledge and abilities and is satisfied with performance, he/she is more receptive to elevate apprentice staff to qualified “physician extenders”. This status comes with a willingness by the physician to assign them more significant hands-on work, such as preparing injections, taking initial patient histories, orthotic/AFO casting and dispensing, measuring and fitting patients for Diabetic shoes, fitting pneumatic boots, night splints, ankle braces, foot padding and foot/ankle strappings.
If the “right” staff are hired and properly trained, utilizing them as physician extenders adds a whole new level of productivity to the practice without added pressure on the physician. DPMs can spend more of their new-found productive time performing high level podiatric care while their qualified staff/techs manage other patient/practice obligations.
Delegation is a time management strategy that involves letting go of tasks others prove they can handle. It is not shifting work because you don’t want to do it, it’s too difficult or too boring. Delegation takes non-essential tasks off your plate while maintaining patient flow and complimented by simultaneous streams of revenue.
Beware of reverse delegation
Reverse delegation occurs when the physician (or manager) assigns a job to an employee, and for whatever reason (lack of confidence, motivation, skill) ends up taking it back, relieving the employee of any associated responsibility. This isn’t helpful for either party long term. It only increases the delegator’s work load and the employee never learns if they keep getting bailed out. If at first they don’t succeed, praise their efforts and encourage try, try again, using a new approach.
Staff can play an integral role in patient care by being the Eyes & Ears of your Practice
There are so many things your staff observe that you cannot because you are patient-occupied. Instructing them to say something when they see (or hear) something should be normal office procedure.
What happens, for instance, when the patient confides in staff by sharing information they were apprehensive to tell the doctor? (They often do!) How about when staff witness unusual walking hardships in a patient who was scheduled for an ingrown toe nail as they escort them into the treatment room? Or when a patient needs assistance getting up and out of their chair? Or when the patient with Diabetes inquiries about what kind of shoes they should wear or how to best care for their feet? These types of observations and friendly staff-patient dialogues should automatically jumpstart a particular protocol.
Let’s say the staff understands that a patient unsteady on their feet is a likely candidate for a “falls risk assessment.” In this case, protocol might dictate they perform a preliminary “Timed Up and GO” test; followed by informing the doctor who may want to initiate a thorough examination on the spot or reschedule it. Maybe the exam leads to the recommendation of an AFO device to control their instability and maybe not. Isn’t it in your patient’s best interest to find out?
Or, perhaps there should be a written protocol stating that non-compliant comments made by the patient to the staff must always be documented in that patient’s chart for the doctor to review. (“I know the doctor told me not to walk on my surgical foot, but, shhhh, don’t tell him I went shopping yesterday.”)
Staff can move towards helping to educate the elderly patient who has Diabetes by giving them a brochure describing preventative foot care; then ready a CDFE form for the DPM. If the practice participates in Medicare’s Therapeutic Shoe Program, exam findings might set in motion a doctor-patient conversation about shoes.
Training your staff to be alert to early signs and knowing what to do before the DPM even enters the treatment room enhances patient care and captures opportunities for the practice (that might otherwise be missed). Protocol in action.
Speaking of Protocol
Structured protocols and policies that are established and routinely enforced can help your practice stay organized and run efficiently and purposely, as if on autopilot. Even on the busy days; I mean, especially on the busy days. And just think…all they do is decrease mistakes, limit repetitive decision making, minimize stress, save time and boost profits. Who knew?
Clinical Treatment Protocols – Thanks but no thanks?
When it comes to treatment protocols, some physicians resist this approach to care as “too rigid” and favor the flexibility to “change things up” with each patient. To be clear, visit-to-visit protocols are not intended to lock the physician into just one treatment plan per condition. The advantages (noted above) are valuable to our individual practices and in fact are applicable in most any business.
Take the airline industry, for example. Pilots rely on flight plans (protocol) to get their aircraft and passengers safely from one location to another. However if conditions (weather, passenger illness, emergency) warrants changing course, the captain decides, based on training and experience, to communicate with air traffic control and “divert from protocol”, aka the original flight plan. Can you say “Sully” Miracle on the Hudson?
In healthcare, we understand that each patient is unique and to think that one uniform treatment plan can work across the board for every patient is impractical. They expect and are entitled to individualized care and attention. Therefore, it goes without saying that if a heel pain patient’s clinical indications do not warrant an injection, night splint or prescription, even though that may be the established procedure in your practice, “divert from protocol” is always an option. Objective and subjective findings, the patient’s medical history, their response to previous treatment and your expertise will always remain the criteria for patient management.
It’s more constructive to look at clinical treatment protocols as a safeguard mechanism rather than “rigid” boilerplate care. Following a structured guideline makes it less likely to overlook associated services such as DME, supplies, and products that effectively pair with a particular procedure; services you have determined to be most beneficial in comprehensive patient care. Do these preferred services get passed over because it is late in the day and you feel rushed, tired, sidetracked or just plain forget to address them during your patient presentation? If and when that happens, everyone loses. We are aiming for win/win.
Added Bonus
Be aware that by keeping staff actively involved in treatment protocols, there is a management bonus. Back office staff are more anticipatory of the necessary supplies and instrumentation needed in their patient/treatment room prep. Front desk staff learn to coordinate protocols into the schedule. Collectively, their actions improve patient flow, cause fewer interruptions and help keep schedules on-time.
Work Smarter – and Be Profitable
You hold the brush that paints your future. If you’re ready to start somewhere...why not here? A word of advice: Encourage staff participation. Invite them to share their unique perspective and contributions. It is invaluable.
· Initiate a recall program – if nothing else, for orthotic and shoe patients;
· Monitor write-offs and examine account receivable reports for unusual trends;
· Don’t alter treatment recommendations based on your assumption of patients’ finances. Recommend the treatment that they will most benefit from and let them make their own economic decision;
· Work towards a level of efficiency that exemplifies the type of practice where you would like to be a patient;
· Hire a qualified office manager (preferably not family or current medical assistant fill-in).
And, to recap:
· Reduce the number of decisions you make on a daily basis by setting up SOPs that will minimize unnecessary decisions and demand less of your time;
· Make your more difficult decisions and schedule more difficult patients in the AM, before decision fatigue has a chance to set in;
· Weed out needless decisions – Don’t lose all your marbles!
· Identify valuable/productive time and use it wisely Physicians should only perform higher levels of podiatric care, revenue work;
· Train staff as physician extenders, delegate workload appropriately;
· Create solid written treatment protocols to promote consistency, greater staff productivity, comprehensive patient care and increased profitability;
· Don’t tire yourself out by overbooking the schedule; allow more patient time for more comprehensive care and to capture missed clinical opportunities;
· Put employee policies (behaviors, expectations and general guidelines) in writing to avoid addressing them on a recurrent basis and so that the entire team knows the rules and consequences. (Established staff policies and protocol require less management);
· Encourage staff to “see something; say something” and jump start associated treatment protocol.
· Don’t eat the whole elephant in one bite!
You will face a lot of tough choices in your life and in your practice. But guess what? “Your life is a result of your choices. Your choices are your responsibility. If you want things to change, you will change them.” MeditatingMonkeys.com


